
Challenge
Encourage behaviour change among agricultural workers in preventing and seeking treatment for Schistosomiasis
role
User research
Story strategy
Art direction
Prototyping
Outcome
Schistoria, a tailored campaign to inform on effects of Schistosomiasis and promote health seeking habits
client
Merck
Dalberg Media
tools
Miro
Canva
Figma
Google Workspace
when
7th – 29th
January 2021
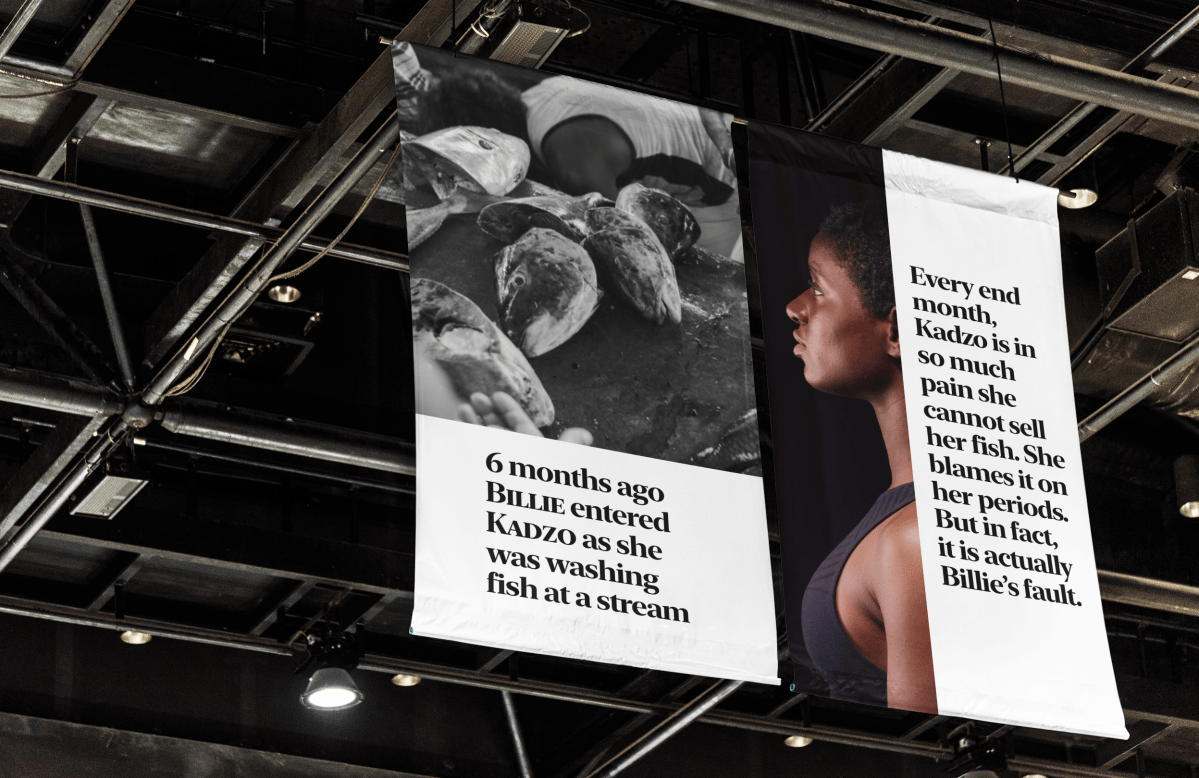
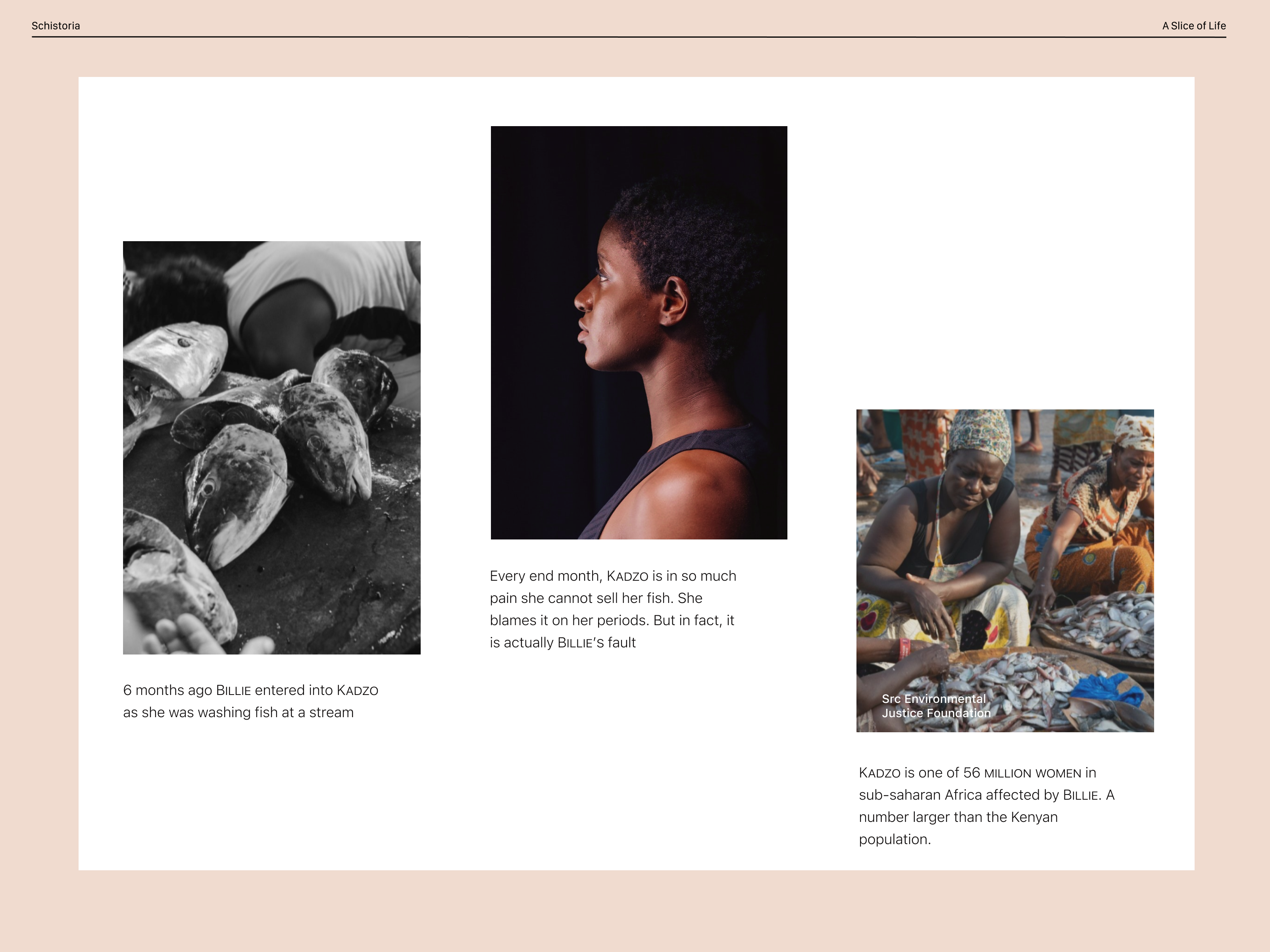
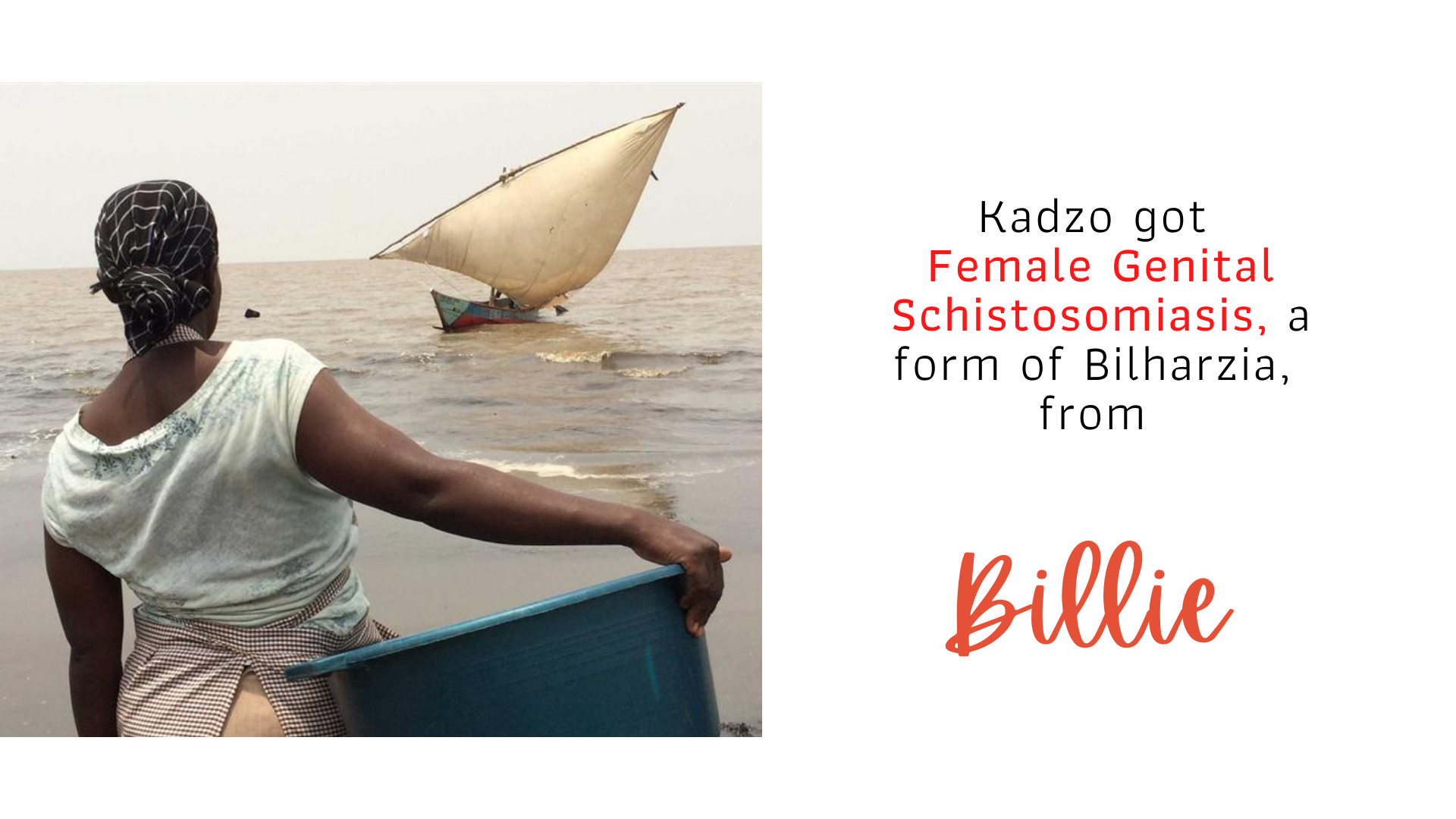
When Kadzo got married, she never suspected that there was an insidious creature hiding inside her. She came from a respectable nuclear family and had a modest means of livelihood as a fishmonger. The only clue was perhaps the irregular, somewhat painful periods she’d been having nine months to her wedding.
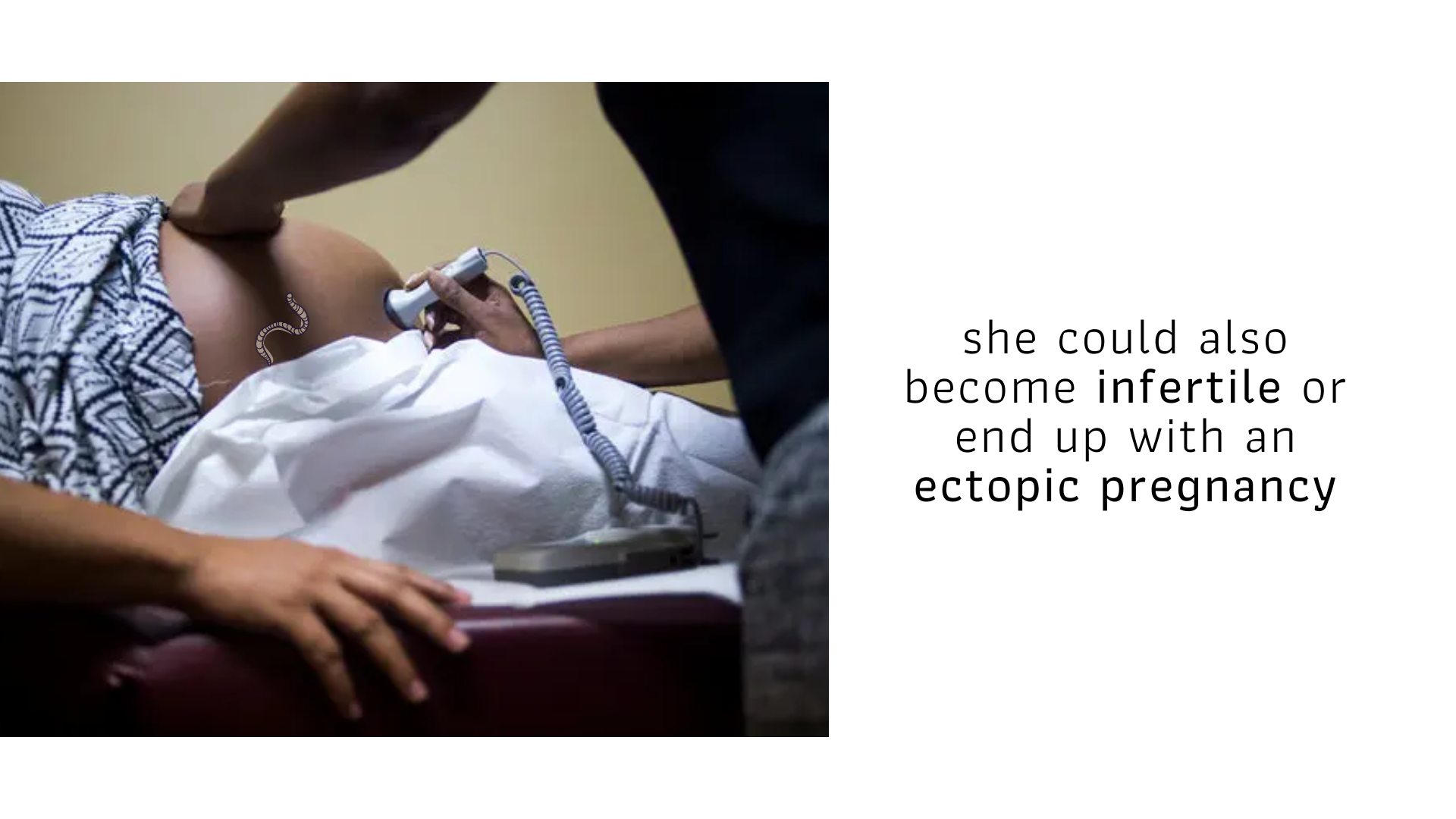
A few months after she tied the knot in a colourful traditional coastal ceremony, Kadzo discovered she was pregnant. Four weeks into the pregnancy, while cleaning fish in her stall by the dam, she started experiencing severe pain on one side of her abdomen. The last she remembers is seeing blood trickle down her calf.
Her fellow fishmongers said they’d found her slumped over her half-gutted fish, unconscious. At the district hospital, a conscious Kadzo was informed that she’d had an ectopic pregnancy and in order to safeguard her life, she required a laparotomy – removing the embryo and repairing any internal damage to the fallopian tubes.
And that’s how Kadzo lost her first child; to Billie, the creature that had been slowly destroying her. She has since had recurring reproductive problems that are affecting her future fertility.
While researching Billie (schistosomiasis, bilharzia or snail fever) and its effects in Kenya, we encountered many different versions of Kadzo’s story. According to the World Health Organization (WHO), over 80% of schistosomiasis cases are found in sub-Saharan Africa. The organization has placed schistosomiasis as the third most devastating tropical disease, following malaria and intestinal helminthiasis. Schistosomiasis continues to seriously affect local communities in Kenya, with a particularly severe impact on women of child-bearing age who suffer considerably from female genital schistosomiasis that causes menstrual disorders, preterm labor, anemia, and infertility.
Merck, a leading science and technology company, in partnership with WHO committed to tackle bilharzia and has already donated 1.3 billion tablets of praziquantel, the treatment for Bilharzia. Kenya has been one of the recipient countries since 2011 and has been provided with 19.7 million praziquantel tablets to date. Together with Dalberg, a mission-driven communications and experience consultancy, Merck sought to combine its efforts in provision of treatment, with innovative human-centered health education. The Bilharzia Storytelling Lab, a result of this collaboration, gave birth to Schistoria, a story making effort aimed at raising awareness on the causes of bilharzia, its effects on women and ways to seek treatment and prevent its recurrence.
Schistoria was designed as an experience ecosystem that supports a female agricultural worker’s journey, from her initial awareness of female genital schistosomiasis to anonymously self-checking for symptoms, to accessing a health facility for testing and possible treatment and future prevention education.


Schistoria comes as an approach to transform bilharzia from an ailment necessitating a prescription (a piece of paper that is handed to you by a doctor) into a conversation (a program that ensures you become aware of how it affects you, seek treatment for it, and continually engage in activities to prevent re-infection). It acts as a vehicle for behavioral change that’s flexible, with room to grow into a much larger movement.

Outcome
2/6
Schistoria was the runner up project that came out of the 2021 Bilharzia Storytelling Lab. Funding to match the USD 10.000 won by the first placed team was promised by Merck and partners for a mini-pilot in Kwale.
Recognition
“At Merck, we do not limit our commitment to providing treatment alone. The Storytelling Lab is the next important step in upscaling our activities in the prevention of infection with bilharzia through health education.”
Read more
Why Schistoria?
Once the team was presented with the design challenge, we asked ourselves, “What do we know about Bilharzia?” The question allowed us to recognize and build up on our existing knowledge and freely focus on what we did not know.
What we knew
There are specific demographics and locations that experience a higher risk of contracting and experiencing the negative effects of Bilharzia than others.
Agricultural workers
Engaged in occupations involving contact with infested water.
School-age children
Living in endemic areas.
Domestic workers
Particularly women doing tasks that involve the use of infested water.
Our risk-group of female fishmongers fell at the intersection of domestic and agricultural workers.
What we did not know
- What female fishmongers do, think or feel about Bilharzia.
- If and how female fishmongers value health offerings.
- Whether there have been challenges to implementation of existing solutions.
- What the future needs of female fishmongers residing in endemic areas may be.
In order to come up with answers to our gaps in knowledge, we proceeded to identify people to speak with. Through appropriate contacts within the team and our partners Dalberg Media and Merck, we were able to speak with:
4
Agricultural & domestic workers
2
Community health workers & volunteers
2
Community leaders
2
NTD experts
NTD -> NEGLECTED TROPICAL DISEASE

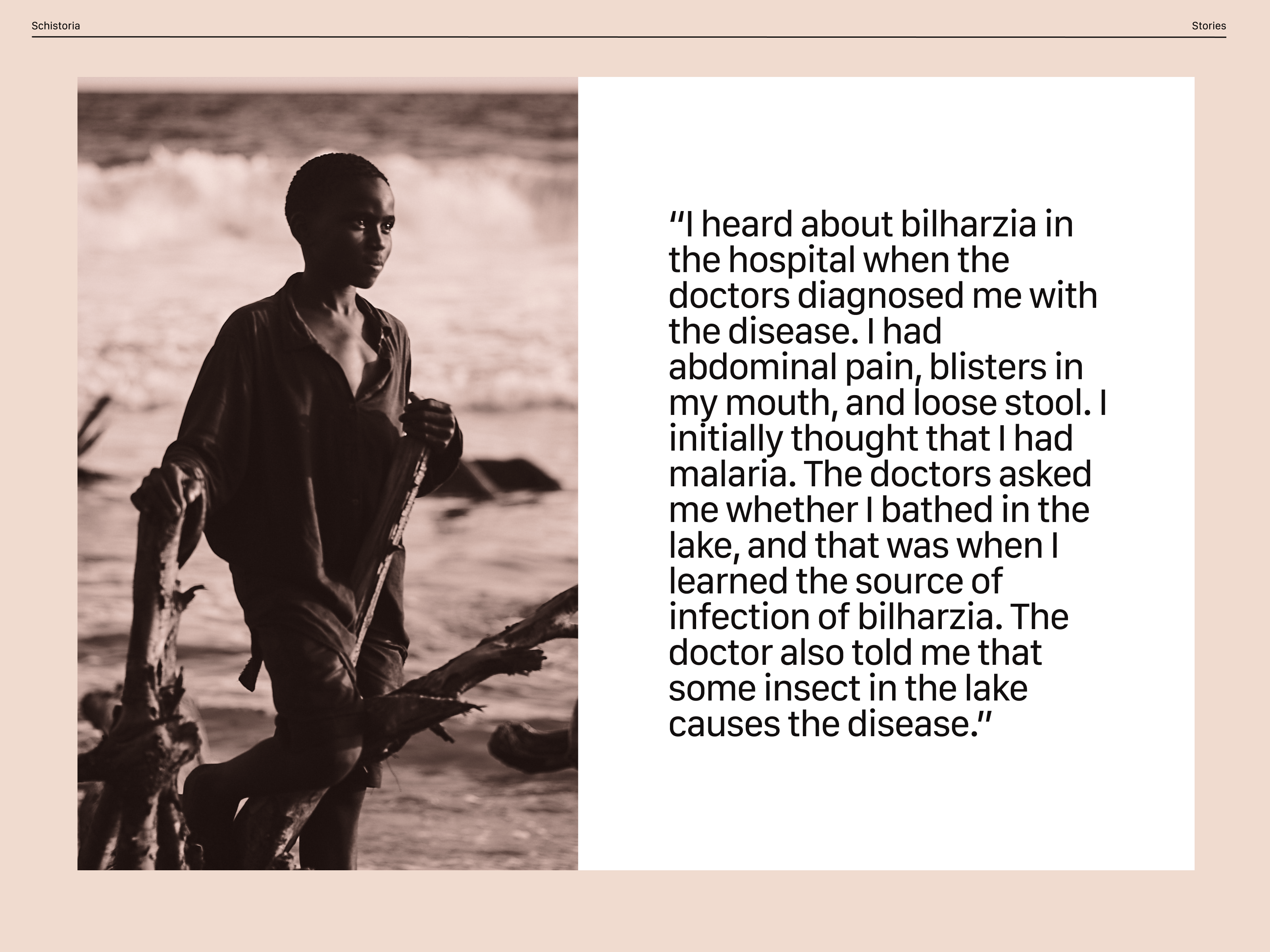
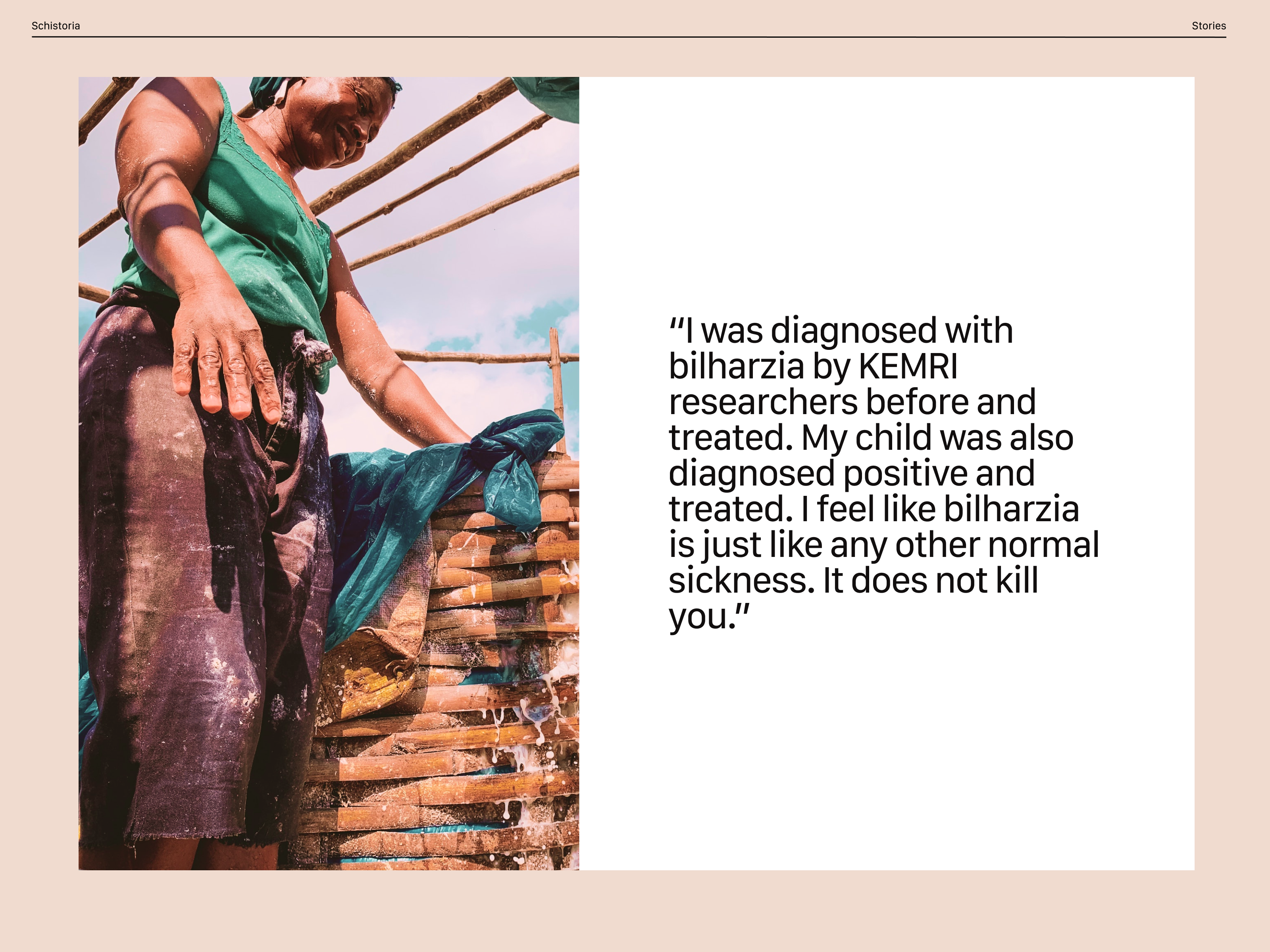
Listening to their stories and gaining inspiration from them
The project started in the first quarter of 2021, and therefore given COVID 19 restrictions, all research had to be done remotely. The methods we employed were:
individual interviews
Virtual interviews enabled us gain a rich view into the behaviours, reasoning and lives of the agricultural workers.
secondary sources
Research reports, papers, journal entries and media articles focusing on the Eastern African neglected tropical diseases space available online.
expert interviews
Contacts provided through our partners and the Ministry of Health enabled us to learn a large amount about the problem space in a short period of time.
In developing an interview approach, there was a need to strike a balance between getting relevant information and engaging with our respondents as a curious friend. Therefore, we began by brainstorming topical ideas we’d like to cover during the interviews. We came up with these broad areas of questioning:
sources of livelihood
access to water and sanitation
health financing mechanisms
sources of information on bilharzia
extent of knowledge on bilharzia
attitudes on prevention and treatment
We then used virtual post-its on Miro to capture questions that respond to these topics, e.g., for sources of information we would ask: “Have you heard about ways Bilharzia is transmitted?”
More of such questions informed the discussion guide, which opened with specific questions about household demographics and stories of recent health concerns; it then went broad looking for respondents’ aspirations for the future and experiences with the health system. The guide then probed deep into their income sources, and other questions specific to the innovation challenge.

Translating stories into opportunities, solutions and prototypes.
In this phase, we took on empathetic approaches in an effort to not just understand the problem mentally, but to start creating solutions from a connection to the risk group’s actual thoughts and feelings.
We started by sharing what we heard and gleaned from the virtual field and desk research as relates to the topical ideas we had outlined: life history, household details, income, aspirations, and information on bilharzia.
With stories from the field all laid out, we began looking for themes and larger relationships between them. Some revelations that made us sit up and pay attention were:

We concluded that there is a lack of awareness and limited access to wholesome education on Bilharzia. Therefore, there needs to be increased awareness regarding the serious health implications of Bilharzia acquisition, especially for women.
In order to ideate solutions for this uncovering, we prepared for a brainstorm by rearticulating the problems and needs we had uncovered in a future-facing way. We asked ourselves:
How might we better inform women on the adverse effects of Female Genital Schistosomiasis?
With the above opportunity area acting as the basis for brainstorming, we came up with a variety of solution ideas. With dot-voting, we surfaced the most promising ideas, which started an internal dialogue about how the ideas would work and approaches we would use to externally communicate to our partners.
With decisions from this stage, we went into prototyping with two of the most voted for solution ideas – a picture story and a self-check USSD code.
Early Schistoria concepts


Testing
Going back to the people, or a subset of the people you talked to and walking them through your solutions is crucial to understanding what may need to change or be improved. We did a few run throughs with:
health workers
Voluteers based in Kwale county.
dalberg Mentors
Resident mentors at Dalberg Media.
health ministry
Ministry of Health officials.
The feedback we received from them made us rethink and redesign the two artefacts into an experience that takes on a more conversational tone, which we postulated would be more effective than a clinical, authoritative one.
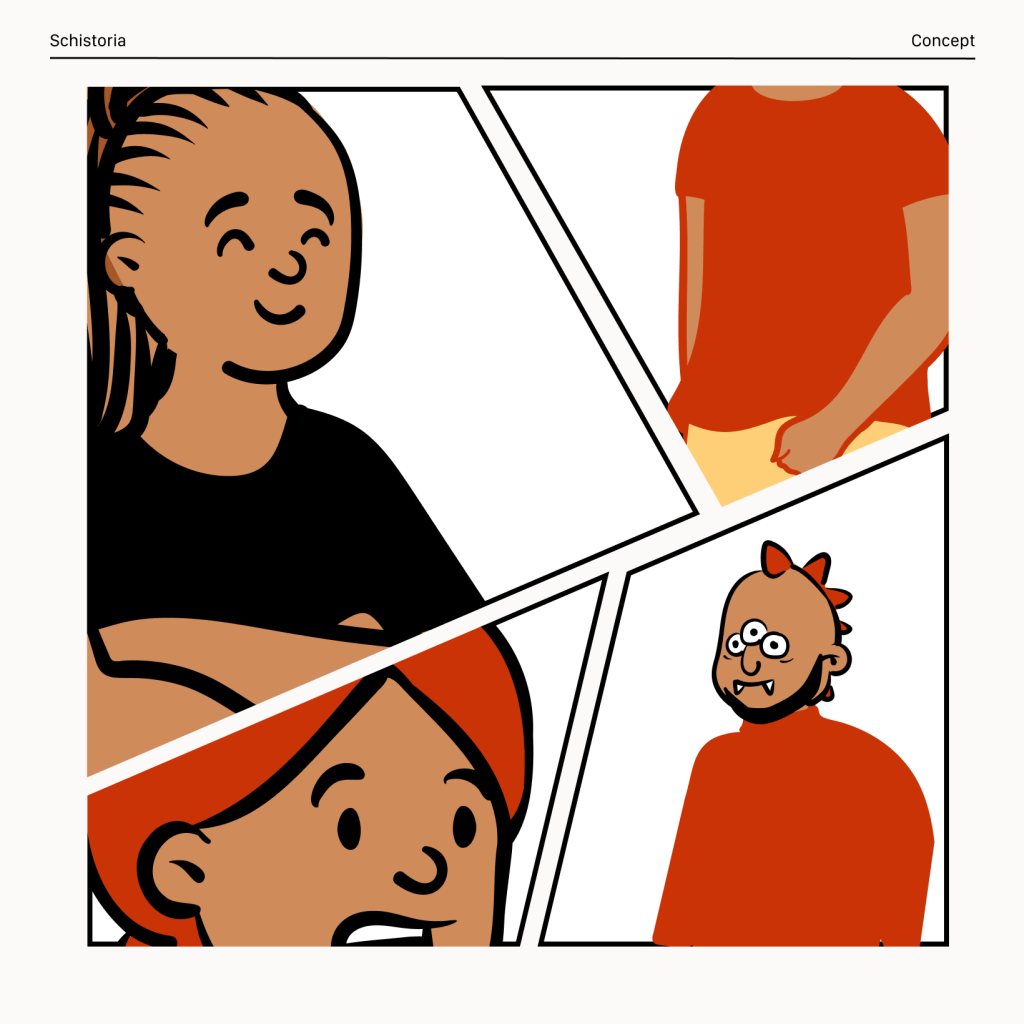
A comic strip representing the characterisation and action flow for Schistoria. 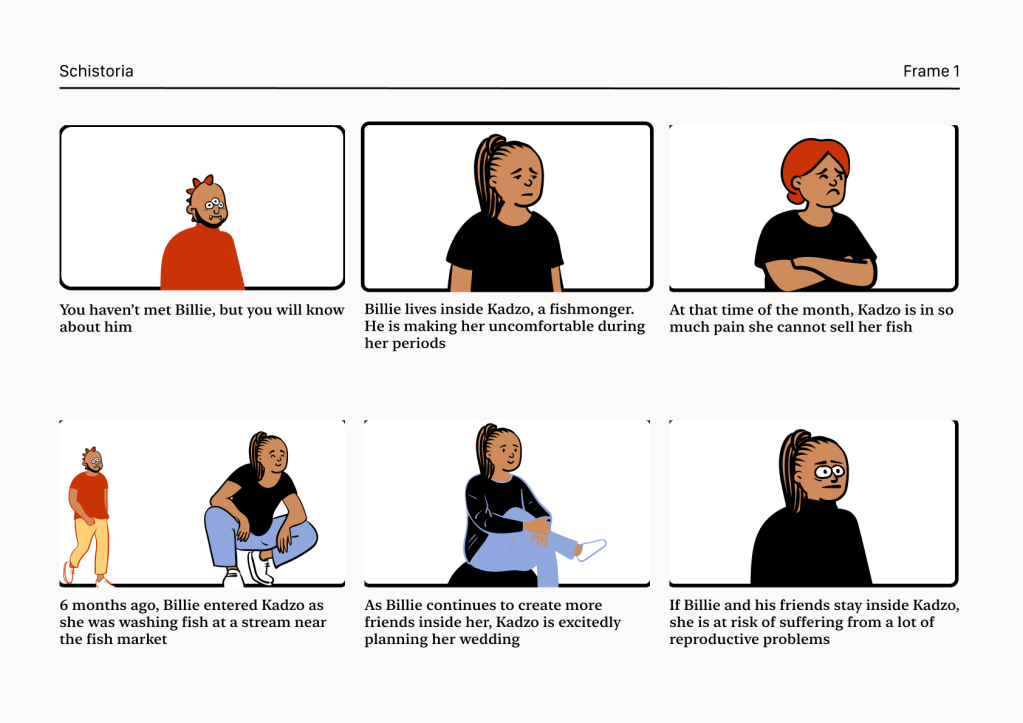
Revised textual messaging for Schistoria (EN).

Ensuring sustainability over the long term.
Implementation of Schistoria will be an iterative process that will likely require many prototypes, mini-pilots, and pilots to perfect the solution and support system around it. We are therefore taking on a tempered, stepwise approach.
Step 1: A Sustainable Revenue Model
Given the high costs of setting up and maintaining a USSD code, we’ve started exploring avenues through which proposals to partners can help subsidize the costs, if seen from a corporate social responsibility angle. Such an offering would ensure we pass little to no costs to the women intended to use the service.
Coupling our approach with funding support from Merck and The End Fund channelled towards refining the language, communication and characterisation of Schistoria, resulting behavioural change would hopefully start setting in within the first two years of implementation.
Step 2: Capabilities Required
We asked ourselves, what channels would we use to distribute Schistoria?
Beach Management Units
Offer physical spaces for meetings, training and mounting the picture story.
Chamaa Leaders
Encourage members to attend chamaa meetings featuring CHVs.
cHVS & chrS
Act to inform on Bilharzia, educate on the use of the USSD code, support health facility referrals, and follow-up post clinical visits.
local authorities
A source for permits to publicly mount picture stories, provide local guides and fixers, mobilize locals, and provide security where necessary.
What human, manufacturing and technological capabilities are required to deliver this solution?


ux RESEARCH & dESIGN
User experience research, writing and design by mwaniki nyaga, eunice kilonzo & fender madegwa
ussd dEVELOPMENT
Contract a software developer and work alongside Safaricom’s Technology for Development team.

BRANDING & ADVERTISING
Ranzwett for printing of designed assets and social influencing within identified mini-pilot locations.
What organizations or individuals have capabilities that we do not?
safaricom
Technology for Development team as a CSR partner on USSD cost subsidy.
UNES health it
Provision of health facility databases for recommendations and contact details.

health ministry
Community advisors to help identify a target audience for field user-testing of Schistoria.

fishing contractors
Donation of equipment and infrastructure that would improve fish-handling hygiene.
Step 3: Metrics for Success
How will we know if our solutions are yielding their intended results? Here, we need to go back to our theory of change.
“Addressing issues of communication and information will establish more aware and better educated agricultural workers, setting off a chain reaction resulting in the elimination of schistosomiasis as a disease in many endemic areas.”
Schistoria’s theory of change
In order to know whether we are making meaningful steps towards achieving this change, we needed indicators to keep an eye on.
Awareness
The goal involves people engaging with something new, therefore, we need to know whether we are getting more community members aware of Female Genital Schistosomiasis and its effects. Eventually, the type of impact we are going for is a perceptual shift in women’s attitude to FGS.

Engagement
The goal is to get more women to self examine via USSD and have them seek out timely treatment, if symptomatic. The engagement indicator to track would be how many women are actively seeking out diagnosis and treatment for FGS.
In summary, for the DELIVER phase of Schistoria, we will need to conduct mini-pilots leveraging our capabilities and tracking the aforementioned indicators. In addition, the team will interview health facility workers and community health volunteers for anecdotal evidence of behaviour change and assess the success of the program with a participatory co-design approach.
After the mini-pilot, a large scale pilot may kick into gear. The pilot will eventually include tracking of statistical evidence such as the rate of decline in FGS diagnoses or rate of increase of FGS testing by women in the endemic localities.
